The Only Guide for Dementia Fall Risk
The Only Guide for Dementia Fall Risk
Blog Article
4 Simple Techniques For Dementia Fall Risk
Table of Contents5 Easy Facts About Dementia Fall Risk ShownThe smart Trick of Dementia Fall Risk That Nobody is DiscussingDementia Fall Risk Things To Know Before You Get ThisThe Main Principles Of Dementia Fall Risk
A fall risk evaluation checks to see exactly how most likely it is that you will certainly drop. The analysis usually includes: This includes a series of concerns concerning your overall health and if you've had previous falls or issues with balance, standing, and/or strolling.Treatments are suggestions that might lower your danger of falling. STEADI consists of three actions: you for your danger of dropping for your threat aspects that can be enhanced to try to avoid drops (for example, balance troubles, impaired vision) to lower your danger of falling by making use of effective approaches (for instance, providing education and resources), you may be asked a number of questions including: Have you dropped in the previous year? Are you worried regarding falling?
After that you'll take a seat once again. Your company will examine the length of time it takes you to do this. If it takes you 12 seconds or even more, it may indicate you are at greater threat for an autumn. This examination checks strength and equilibrium. You'll being in a chair with your arms went across over your upper body.
Relocate one foot halfway onward, so the instep is touching the big toe of your various other foot. Move one foot completely in front of the various other, so the toes are touching the heel of your various other foot.
The smart Trick of Dementia Fall Risk That Nobody is Talking About
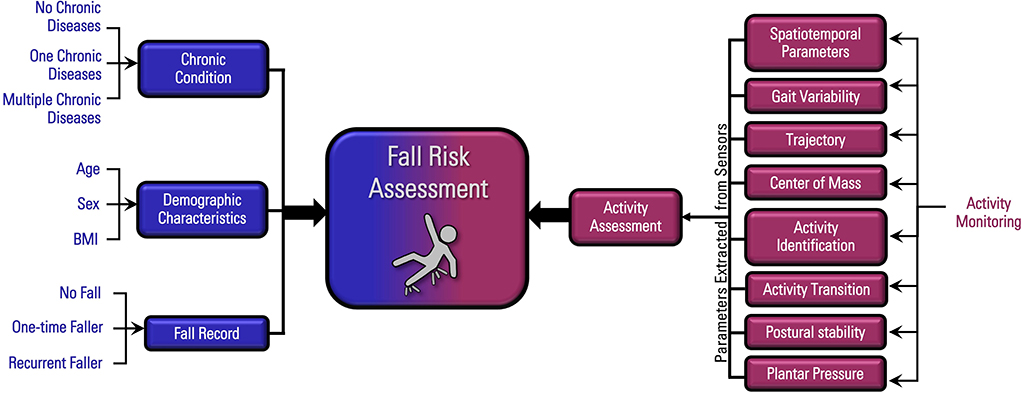
The majority of drops take place as an outcome of several contributing elements; as a result, taking care of the danger of dropping starts with determining the elements that add to drop risk - Dementia Fall Risk. Some of the most relevant threat factors include: History of previous fallsChronic medical conditionsAcute illnessImpaired gait and balance, reduced extremity weaknessCognitive impairmentChanges in visionCertain high-risk medicines and polypharmacyEnvironmental elements can additionally raise the danger for falls, consisting of: Insufficient lightingUneven or harmed flooringWet or slippery floorsMissing or harmed handrails and order barsDamaged or incorrectly fitted tools, such as beds, mobility devices, or walkersImproper usage of assistive devicesInadequate supervision of the individuals staying in the NF, including those who show aggressive behaviorsA successful autumn risk administration program needs a complete professional evaluation, with input from all participants of the interdisciplinary team
The treatment plan need to additionally consist of interventions that are system-based, such as those that promote a secure setting (suitable lights, handrails, order bars, etc). The performance of the interventions should be examined periodically, and the care strategy revised as essential to reflect modifications in the fall danger assessment. Implementing an autumn risk administration system using evidence-based best practice can decrease the prevalence of falls in the NF, while restricting the capacity for fall-related injuries.
More About Dementia Fall Risk
The AGS/BGS standard recommends screening all adults aged 65 years and older for autumn danger annually. This screening is composed of asking individuals whether they have dropped 2 or even more times in the past year or looked for clinical interest for Dementia Fall Risk a loss, Discover More Here or, if they have not dropped, whether they feel unstable when walking.
People that have fallen as soon as without injury should have their balance and stride reviewed; those with stride or equilibrium abnormalities must get extra analysis. A background of 1 loss without injury and without gait or equilibrium problems does not warrant more analysis beyond continued annual autumn threat screening. Dementia Fall Risk. A loss risk assessment is required as part of the Welcome to Medicare evaluation

Everything about Dementia Fall Risk
Recording a falls history is one of the top quality signs for loss prevention and administration. Psychoactive drugs in particular are independent predictors of drops.
Postural hypotension can commonly be alleviated by decreasing the dosage of blood pressurelowering drugs and/or stopping medications that have orthostatic hypotension as an adverse effects. Use above-the-knee assistance tube and resting with the head of the bed raised might also decrease postural reductions in blood stress. The preferred aspects of a fall-focused health examination are revealed in Box 1.
A yank time better than or equivalent to 12 secs recommends high autumn risk. The 30-Second Chair Stand test evaluates lower extremity toughness and equilibrium. Being not able to stand from a chair of knee height without using one's arms indicates increased fall risk. The 4-Stage Balance test assesses fixed balance by having the client stand in 4 settings, each progressively extra difficult.
Report this page